By: Jacqueline Russo, RN, DDS
Introduction
Dentistry in the 21st century can be both rewarding and demanding. Dental professionals work in a complex environment that requires high clinical skill levels and staff with high levels competency. Consideration must be given to ergonomics, and long and complex procedures require great attention to detail. In addition, high patient expectations need to be met, and staff and patient management must occur. There are also the demands of running a small business. Time pressures may also result from the drive to (over) maximize efficiency for productivity and profitability.1
The word ‘ergonomics’ is derived from the word ‘ergo’ for work and ‘nomos’ for natural laws or systems. Ergonomics is frequently discussed in the context of work-related musculoskeletal disorders. Preventing/alleviating these through the use of technical and posture solutions. However, ergonomics encompasses physical and psychosocial (mental) stress,2,3 which together cause health issues and professional burnout.
Clinicians’ stress levels have been found to be increased by a number of psychosocial factors, including dealing with uncooperative patients, those with a fear/dislike of treatment, patients with physical disability, postponed/cancelled appointments, lack of case acceptance, time and schedule constraints and dealing with staff.4 The World Health Organization and National Institute for Occupational Safety and Health (NIOSH), additionally considered organizational and sociocultural factors to be associated with musculoskeletal disorders (MSDs).5 Ergonomics has been described as ‘the study of the problems of people adjusting to their environment, especially the science that seeks to adapt work or working conditions to suit the worker.’ 6
Occupational Health, Physical Stressors and Injuries in the Dental Office
In one survey on occupational health among dental hygienists, musculoskeletal symptoms were commonplace while psychosocial stressors were found to include social isolation, role identity and conflict. Inadequate breaks also impacted ergonomics.7 The design of an ergonomic dental office is an important element in reducing these, and creating a healthy and productive work environment.6 Flow, function, ergonomics and aesthetics are all a part of it.
Physical stressors among dental personnel, including dentists, dental hygienists and dental assistants, place them at occupational risk for musculoskeletal disorders of the neck, wrist (carpal tunnel syndrome), elbow, hand, shoulder and back. MSDs impact work hours and productivity. In the mid-1990s, almost one-third of dentists in a British study reported retiring early due to occupation-related MSDs.8 In a 2005 survey of dental hygienists in the United States, MSDs resulted in 27% reporting that they had reduced work hours. The most common affliction was hand/wrist pain.9
Numerous studies have reported on the prevalence of MSDs in dental healthcare workers. Significant numbers of dentists in numerous international studies have reported MSDs and pain. Across studies in different countries, conducted between 1998 and 2007, 20% to 57% reported neck pain, 8% to 52% reported shoulder pain and 45% to 60% reported lower back pain.10-14 (Figure 1)
In one study, dental hygienists were found to be most affected, with 66% reporting neck pain and 53% reporting shoulder pain. For dentists and dental assistants, the prevalence was 41% and 30%, respectively, for neck pain and 30% and 24% for shoulder pain.15 (Figure 2)
Repetitive movement, straining, movement with excessive force such as during manual scaling, limited motion, reaching too far, arms above the shoulders, repeatedly reaching up, bending the neck, forward head posture, twisting, poor visualization- and poor/awkward posture are all risk factors for MSDs and pain.16,17 Not having proper chairs or not positioning chairs in the correct way, cabinets at the wrong height or distance from the staff member, and items placed at the incorrect height or area all increase poor posture and functioning. This increases the risk for MSDs. The placement of the dental team, where and how people sit or stand at a chair, their equipment, and their materials become critical so that human ergonomics is achieved. Instrumentation also plays a role, providing an opportunity to change out to more ergonomic devices. (Table 1)
Ergonomic Solutions in the Dental Operatory
Four-handed dentistry,18 improved work posture and practices can improve ergonomics. Four-handed dentistry results in organized and collaborative performance of work, effectiveness, increased productivity and efficiency. It has been shown to reduce the risk of elbow and forearm discomfort associated with dentistry, possibly due to easier instrument handling and less reaching.5
Devices and Instrumentation
Utilizing devices that reduce repetitive motions, required force, pinching, tight grips and poor visualization all aid ergonomics. Examples include fiber-optic lighting, the use of ultrasonic scalers more than manual scalers, wide-handled grips on instruments and functionally designed handles are all examples. Considerations in selecting equipment/devices include the handle and overall shape and size, weight, balance, and the ability and ease of use.
Work Posture and Function
Improved work posture includes working with the elbows lower than shoulders, consistently using mirrors, loupes, and indirect vision instead of bending to achieve visual access, adjusting the patient’s chair and asking the patient to adjust his/her position (e.g., turning the head to the left or right to aid access to a particular quadrant/ clinical site) can help to improve posture.5,19 In addition, client chair designs that improve access and lessen distance between the clinician and the patient are ergonomically sound. Design strategies include chairs with thin back and headrest, narrow chairs, and adjustable headrests.20,21 (Figure 3)
Operatory Design and Ergonomics
Improvements in dental operatory design, operatory furniture and instruments can help provide ergonomic solutions and reduce the risk of work-related stress and injuries.17
In four-handed dentistry, the dentist or dental hygienists spend the majority of their time working intraorally, while the dental assistant should be performing 80% to 90% of the remaining work in the operatory. Therefore, the clinician will usually be in the 9 to 12 o’clock position (assuming he/she is right-handed), mostly 11 to 11:30, and should be seated with the stool down at its lowest setting. Based on an NIOSH and Indian Health Services survey, sitting in the 11 to 11:30 position results in fewer back injuries than the 9 to 10 position.20 The operatory dimension is best designed around the functional movements of the dental assistant, rather than the dentist. The assistant should be up high enough to be able to see without leaning over, with the left hip adjacent within a few inches of the patient’s left shoulder, and the assistant’s eye level should be 6 to 8 inches above the clinician’s eye level. Ergonomic four-handed dentistry treatment positions provide for the largest and most efficient working plane from a seated position. Conversely, working with your arms up gives the smallest and least efficient working plane.
There are basically three types of delivery units. With the single unit, one unit serves both the clinician and the assistant. The over-the-patient (or trans-thorax) unit again consists of one unit that serves both the clinician and the assistant, and it is positioned over the patient’s chest. The third option is the dual unit, or split system, which means there’s a unit in the back for the assistant, and one for the doctor that either comes off the side wall, or one that comes over the chest of the patient. Over-the-patient equipment reduces twisting and turning required to access devices and equipment.20
Dimensions in Operatory
The dimensions within the operatory are key. In the concept of dental office design, there are two major criteria. It has to function, first and foremost, and no matter what kind of high tech equipment is available, if it gets in the way of your primary function of providing high quality dental care to people, it does not fulfill requirements. Operatory dimensions are important for efficiency and ergonomics. Ideally, the distance between the arm of the chair and the edge of the side cabinet should be approximately 27 inches, making it possible for the assistant to comfortably reach essentially all of that area. The same distance is optimal to the rear wall or cabinet. A distance of 6.5’ to 7’ across is the optimum dimension from the leading surface of one cabinet to the leading surface of the other. This dimension allows you to work effectively, and for either person on the operative team to be able to reach just about anything they want on these side cabinets, without any extreme movements. The depth of the side cabinets can vary between 15” and 18.” The end result is a 9.5’ to 10’ room. (Figure 4)
Zones in the Operatory
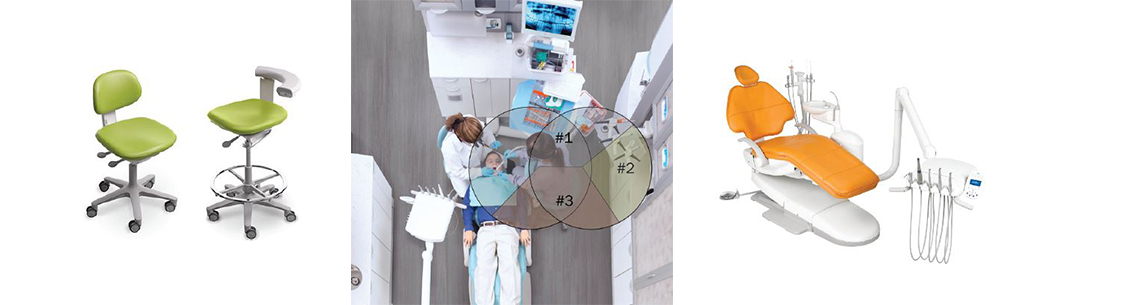
Zones/zoning within the operatory based on types of required movement is an important concept. Two circles forming radii around the assistant create the zone within which the assistant can reach everything by only doing class 4 movements or less. Class 1 movements are ergonomically the most favorable, and Class 5 the least favorable with reaching, twisting and turning. The design should be such that clinician movements are limited as much as possible to classes 1 through 3, and dental assistant movements to classes 1 through 4. (Figure 5)
The primary area is area one, the primary work space where instrument transfer occurs, static and dynamic instruments are arranged and laid out for use, and access is provided to a drawer that would carry additional consumables to replace those items that get routinely used up on the tray or on the cassette. The dental assistant can easily reach anything within this primary area. Area two is a secondary work space. Here, the assistant can turn 90 degrees, without exceeding class 3 and class 4 movements, to mix and do those things that occur only occasionally during a procedure. Area three is the most remote within the zoned area, for use infrequently and cannot be accessed without undesirable class 5 movements.
Operatory Stools
Investing in comfortable chairs with sufficient adjustments is essential. Purchasing cheaper stools with few adjustments, and that cannot tilt, makes it difficult or impossible to find an ergonomic position. Adequate lumbar support at the back is crucial, while a chair back extending above where lumbar support is required is just cosmetic. Good lumbar support has been shown to reduce the risk of lower back pain and to promote good posture when sitting.5 Consistent lumbar support helps to prevent lower back pain, and is provided in stools that help foster a seating position compatible with lower back anatomy. (Figure 6) It also limits undesirable twisting and reaching, which falls under Class 4 and 5 movements. In addition to a stool with good lumbar support for the clinician and dental assistant, the height of the stool must be considered.17,22 The clinician’s stool should result in the clinician’s thighs being parallel to the floor, and provide full seat coverage. The dental assistant’s stool should ideally have a foot ring to rest the feet on and a taller center shaft than the clinician’s stool, so that it can be positioned with the assistant ergonomically seated higher than the clinician. 23 (Figure 6) It is also important the operator adjust the armrest to provide elbow support, thereby reducing neck and shoulder strain.
Lighting and Magnification
Good lighting is essential. Poor lighting is responsible for awkward positions, poor posture, and Class 4 and 5 movements including twisting and turning. Ambient light should be good as a baseline, and additional lighting is required to improve visualization. Over-chair lighting should be readily accessible without stretching, fiber-optic lights on handpieces concentrate light on the clinical site, and hand mirrors can be manipulated to assist with lighting. In addition, the use of loupes and chairside microscopy improves visualization and therefore ergonomics, helping to encourage good posture, avoid forward posture (slumping) and maintain forward flexion of the neck under 20 degrees.22,24 (Figure 7)
The ‘Healthy’ Office
The ‘healthy office’ is designed for the health of clinicians, dental assistants and other staff. The principles of flow in various areas of a dental office, whether it’s operatory, bay or whatever part of the dental office, still remain mostly the same. The single biggest factor in reducing stress is having the office properly zoned functionally. Specific activities typically occur only in certain areas, and if they overlap, then efficiency is reduced and repetitive actions increase. There should be as little interface as possible between the public and the treatment zone, and that’s where the overlap part comes in. There should be a buffer zone, which is usually a corridor, of 8 feet or more in length, and typically approximately 4 to 5 feet in width, that joins and connects the treatment and public zones. Windows in the operatories are important, for the clinician, staff and patient to maintain contact with the outdoors visually if at all possible. Particularly for clinicians and dental assistants, who are pretty much locked into that area, the lack of windows can add to stress on the body, mentally and emotionally. Design should also consider the ergonomics of other areas, such as the sterilization area and the laboratory if you have one.
The second major criterion for dental office design is image, which is like the icing on the cake. Esthetics catches everyone’s eye and may help to reduce patient fear and instill trust in the clinician’s abilities. Your office is one of the biggest marketing tools you have, and it’s one of the first opportunities for you to make a good impression. It is often one of the most overlooked areas when it comes to design. (Figure 8)
Other Benefits/Considerations
A healthy office requires a healthy structure. Consumers are more educated than ever about the impact we have on our environment and how our environment impacts our well-being. Designing an environmentally conscious office shows your patients, your peers and the public that you care about their well-being and safety and allows you to take advantage of a number of state and local incentives. Your level of commitment may include selecting paints with low or no volatile organic compounds (VOCs) or extend to getting your space LEED certified. Being green starts at the paint and surface materials and can extend to the mechanical, plumbing and electrical systems and beyond to the structure of your building and even your site. Since the environmental movement is now becoming a requirement in some respects, building codes are being altered for greater energy efficiency. For example, many jurisdictions are only allowing 1 watt per square foot of space. Indoor air quality is crucial in a healthy space, and the more your space has low to no VOCs, formaldehyde and off-gassing, the better.
Conclusions
Ergonomics plays a key role in the health and safety of clinicians, dental assistants and staff. It helps to reduce the risk of MSDs, including those associated with stress/repetitive injuries. Intelligent and efficient office design is important for ergonomics, and therefore for efficiency and functionality. Key elements include the workflow and design of the operatory, device and instrument selection, creating a buffer between treatment and public areas of the office, and determination of elements selected for the healthy office in line with your philosophy. In addition, productivity and profitability can improve when the office functions ergonomically, and staff and patient retention may also improve. The bottom line is that reducing physical, psychosocial and other stressors in the dental office through ergonomic design is not only necessary for the health of everyone in the dental office, it is also good for your bottom line.
ABOUT THE AUTHOR Jacqueline Russo, RN, DDS
Jacqueline Russo’s entire adult life has been dedicated to the study of the human frame, prevention and treatment of disease; helping people live their best possible lives both personally and professionally. She is co-founder of Enviromed Design Group, a Texas-based dental and medical offi ce design company. She and her partners have created functional and aesthetic offi ces all over the country that allow practitioners to love where they work. Jacque is a coach, author, lecturer and key opinion leader who loves teaching and learning from her clients and their experiences. Jacque received her BSc in nursing from Indiana University, her dental degree from Baylor College of Dentistry, and is a certifi ed nutritionist and supplement consultant. She is a Board Member, Vice President and Program Chair of the American Academy of Oral Systemic Health, and a member of the American Academy for Anti-Aging Medicine. She can be reached at Jacque@enviromedgroup.com.
References
1 Mangharam J, McGlothan JD. Ergonomics and dentistry: a literature review. 1998;25- 81. In: Ergonomics and the Dental Care Worker. Washington, DC: American Public Health Association. Murphy DC, editor.
2 Plasschaert AJ. Ergonomics in dental practice. Prevention of physical and mental overload. Ned Tijdschr Tandheelkd. 1999;106(2):46-50
3 Corlett EN, Shipley P. Stressful conditions of work: the participative ergonomics approach. J UOEH. 1989;11 Suppl:541-8.
4 Chaikumarn M. Working conditions and dentists’ attitude towards proprioceptive derivation. JOSE. 2004;10(2):137-146.
5 Khan SA, Chew KY. Effect of working characteristics and taught ergonomics on the prevalence of musculoskeletal disorders amongst dental students. BMC Musculoskeletal Disorders. 2013;14:118.
6 National Maternal and Child Health Resource Center. Facility Design and Construction. Safety Net Dental Clinic Manual, 2011. Available at: https://www.dentalclinicmanual.com/chapt2/1_13.html
7 Crawford L, Gutierrez G, Harber P. Work environment and occupational health of dental hygienists: a qualitative assessment. J Occup Environ Med. 2005;47(6):623-32.
8 Burke FJ, Main JR, Freeman R. The practice of dentistry: an assessment of reasons for premature retirement. Br Dent J. 1997;182(7):250-4
9 Yee T, Crawford L, Harber P. Work environment of dental hygienists. J Occup Environ Med. 2005;47(6):633-9
10 Alexopoulos EC, Stathi IC, Charizani F. Prevalence of musculoskeletal disorders in dentists. BMC Musculoskelet Disord. 2004;5:16.
11 Dong H, Loomer P, Barr A, Laroche C, Young E, Rempel D. The effect of tool handle shape on hand muscle load and pinch force in a simulated dental scaling task. Appl Ergon. 2007;38(5):525-31
12 Finsen L, Christensen H, Bakke M. Musculoskeletal disorders among dentists and variation in dental work. Appl Ergon. 1998;29(2):119-25.
13 Ratzon NZ, Yaros T, Mizlik A, Kanner T. Musculoskeletal symptoms among dentists in relation to work posture. Work. 2000;15(3):153-8.
14 Leggat PA, Smith DR. Musculoskeletal disorders self-reported by dentists in Queensland. Aus Dent J. 2006;51(4):324-7.
15 Morse T, Bruneau H, Dussetschleger J. Musculoskeletal disorders of the neck and shoulder in the dental professions. Work. 2010;35(4):419-29.
16 Valachi B, Valachi K. Mechanisms leading to musculoskeletal disorders in dentistry. J Am Dent Assoc. 2003;134(10):1344-50
17 Murphy DC. Ergonomics and dentistry. NY State Dent J. 1997;63(7):30-4
18 Finkbeiner BL. Four-handed dentistry: instrument transfer. J Contemp Dent Pract. 2001;2(1):57-76
19 Chowanadisai S, Kukiattrakoon B, Yapong B: Occupational health problems of dentists in Southern Thailand. Int Dent J. 2000;50(1):36-40.
20 Indian Health Services. Ergonomics recommendations for dental programs. Available at: https://www.dentalclinicmanual.com/docs/Ergonomic_considerations. pdf.
21 Ahearn DJ, Sanders MJ, Turcotte C. Ergonomic design for dental offices. Work. 2010;35:495-503.
22 Murphy C. Ergonomics and the dental care worker. American Public Health Association, Washington, DC. 1998.
23 Sanders MJ (Ed.). Ergonomics and the management of musculoskeletal disorders, St. Louis, Elsevier Mosby, 2007.
24 Gupta A, Ankola AV, Hebbal M. Dental ergonomics to combat musculoskeletal disorders: a review. JOSE. 2013;19(4):561-571.