By By Walter Chitwood, DDS
There are certain pieces of equipment, like my cell phone, that make me wonder how I ever got through a day before I owned one.
I feel the same way about my Gendex medium-field-of-view CBCT. The convenience of having access to 3D and the information that it produces is priceless. Unquestionably, I would not go back to practicing implant dentistry without the GXCB-500™.
CBCT scans are a very valuable element of an uneventful implant experience. Prior to my investment in 3D, I had to compensate for the inherent distortion of 2D pans; we were never able to truly check trajectory, width, and bone density. Often, I would treatment plan to place a certain size implant. After verifying the case with 3D, larger or smaller diameter implants were actually indicated.
The 3D view dramatically increases acceptance of implant therapy. In the past, the first time that I would present treatment to patients, they would need time to try to understand the concept. Only 25–30 percent made a decision for treatment on the first visit. These days, we are experiencing about a 60 percent acceptance rate on the initial visit, and a
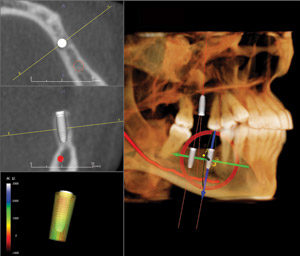
75 percent overall. Why? We are able to show patients their own case in exact 3-dimensional images with implants in place. Prior to 3D, we relied on photos of other completed cases (and their imagination) to describe their procedure and outcome. Now, we are able to show each patient their own case, non-distorted, and in three dimensions. The Anatomage Invivo5 software shows the exact implant location. This creates a clear understanding of the procedure and its benefits to the patient.
Appointment times are also shorter—about 50 minutes from the time the patient is seated until the proposed treatment presentation. Before 3D, it took at least an hour just to gather the information—including a panoramic X-ray, patient examination, study models, etc. We would then reappoint the patient for a report of findings and consultation. For my out-of-town patients, the second appointment was especially inconvenient. Not only do my patients appreciate the convenience of fewer and shorter appointments, my referral doctors are also pleased that we are able to start surgery by the next appointment.
The following case illustrates the benefit of CBCT. We were the third opinion on a possible implant case for a 19-year-old who lost all of his lower teeth and sustained multiple mandibular fractures due to trauma. He had also lost much of his alveolar bone. The first dentist suggested implants and a removable appliance. The second dentist told them that an implant-supported fixed appliance was possible. We were the first to take a CBCT scan, which the patient had never seen, that showed a horizontal void in the symphysis area that had gone undetected by 2D radiography.
The previous two doctors’ plans would have been impossible without initial grafting to create adequate available bone. It would have been a grave surprise for one of the previous dentists to have started surgery, laying the flap for what was supposedly a “routine operation,” only to discover that he had to abort the operation and discuss a bone graft with the patient. CBCT totally transformed the treatment approach and instantly improved the patient’s confidence in our abilities. Rarely a day goes by that we take less than two or three CBCT scans for implant cases. The GXCB-500 gives me invaluable information and communication with patients and colleagues—an integral part of my growing implant practice.